Even if you are convinced of the patient benefits that a remote patient monitoring (RPM) program will deliver, you may still have questions about the financial implications for your organization — and how to best make a program financially worthwhile.
You will need to take a number of essential steps in advance to help ensure the success of the new remote patient monitoring program. These include everything from choosing the RPM system (e.g., Prevounce) that will drive your program to developing an effective mechanism for educating patients on RPM. There is also the not-so-small matter of understanding how you will get paid for your services.
That’s why we have broken down the steps here and provided a quick checklist guide for current remote physiologic monitoring CPT codes. The good news is that, as you will find, building a successful RPM program is fairly straightforward.
Steps to Ensuring Success
Here are four things to know about remote patient monitoring reimbursement.
Coverage of Remote Patient Monitoring
Remote patient monitoring is covered by Medicare. As of April 2022, it's also covered in some form by 30 state Medicaid programs, according to the Center for Connected Health Policy. The organization adds that California and Ohio only cover specific remote physiologic monitoring codes, with payment modeled after CMS reimbursement.
Numerous commercial payers cover remote patient monitoring within their telehealth coverage policies, albeit with some caveats. The number of commercial payers covering RPM experienced a surge due to the COVID-19 pandemic. While coverage of RPM was on the rise prior to COVID-19, and broader coverage for RPM was anticipated in the coming years, the health crisis accelerated this process. As the Kaiser Family Foundation notes, “… many commercial insurers have voluntarily addressed telemedicine [which includes RPM] in their response to COVID-19, focusing on reducing or eliminating cost sharing, broadening coverage of telemedicine, and expanding in-network telemedicine providers.”
Getting Paid for Remote Patient Monitoring
One of your biggest concerns may be wondering what you can expect to get paid for providing remote patient monitoring services. As previously highlighted, RPM is one of the better reimbursing Medicare care management programs.
Here's how remote patient monitoring reimbursement breaks down using average Medicare reimbursement for 2020:
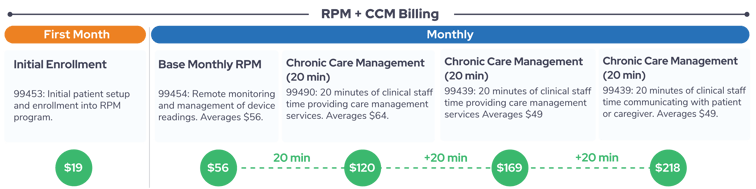
- Medicare pays $19 for initial patient enrollment into a remote patient monitoring program. This includes setup of an RPM device and the delivering of any necessary patient education on using the device and receiving RPM services.
- Medicare provides a base monthly payment of about $56 for monitoring patient data transmitted from the device and ongoing management of the device.
- Medicare provides a monthly payment of about $50 for spending 20 minutes communicating with the patient or a caregiver about the transmitted data and any changes to the care management plan.
- Medicare will provide an additional monthly payment of about $41 if such communication with a patient or caregiver exceeds 20 minutes but is less than 40 minutes. If communication requires 40 or more minutes, Medicare will provide an additional — and final — monthly payment of $41. There are no additional payments for communication taking one hour or longer.

When these reimbursements are added together, the amount a single remote patient monitoring patient can earn an organization up to around $188 per month. More often than not, an organization will typically furnish about 20 minutes of RPM care management per month to a patient, which will bring the total monthly reimbursement to around $106 per Medicare beneficiary.
While $106 may not seem like a substantial amount, as a remote patient monitoring program grows, that $106 per patient quickly adds up. For example, if your organization enrolls 100 patients into your RPM program and each receives the minimum care management services, that will earn you about $127,000 in annual Medicare RPM reimbursement. Even after covering expenses associated, RPM yields significant and — importantly — consistent revenue.
Note: By providing RPM in conjunction with chronic care management (CCM) and other services, all as part of a broader comprehensive care management program, organizations will provide their patients with ongoing care that improves health and wellness while also making a more substantial impact on the bottom line. Learn more about the economics of a comprehensive care management program in this column.
Coding for Remote Patient Monitoring
The next item to consider is how you will receive those payments. You’ll need to ensure that you code your remote patient monitoring services correctly. Let's briefly examine the CPT codes assigned to RPM.
Most of your remote patient monitoring services will be billed under four codes. These codes are often split into two categories: RPM “service codes” — 99453 and 99454 — and timed RPM “management codes” — 99457 and 99458.
The RPM service codes descriptors are as follows:
- CPT 99453 — Remote monitoring of physiologic parameter(s) (e.g., weight, blood pressure, pulse oximetry, respiratory flow rate), initial; set-up and patient education on use of equipment
- CPT 99455 — Remote monitoring of physiologic parameter(s) (e.g., weight, blood pressure, pulse oximetry, respiratory flow rate), initial; device(s) supply with daily recording(s) or programmed alert(s) transmission, for 2-15 daily readings each 30 days.
- CPT 99454 — Remote monitoring of physiologic parameter(s) (e.g., weight, blood pressure, pulse oximetry, respiratory flow rate), initial; device(s) supply with daily recording(s) or programmed alert(s) transmission, for 16 daily readings each 30 days.
The RPM management codes descriptors are as follows:
- CPT 99457 — Remote physiologic monitoring treatment management services, clinical staff/physician/other qualified health care professional time in a calendar month requiring interactive communication with the patient/caregiver during the month; initial 20 minutes
- CPT 99458 — Remote physiologic monitoring treatment management services, clinical staff/physician/other qualified health care professional time in a calendar month requiring interactive communication with the patient/caregiver during the month; additional 20 minutes
The Centers for Medicare & Medicaid Services (CMS) stated that CPT 99457 and CPT 99458 can be furnished by clinical staff under the general supervision of the billing provider. If you’d like more detailed information about remote patient monitoring requirements for billing and coding, download this RPM billing guide.
CMS Guidelines for Remote Patient Monitoring
Perhaps one of the most essential steps in preparing to implement a remote patient monitoring program is to reduce the likelihood of claims denials and avoid scrutiny of your billing practices. To do so, you must understand the CMS guidelines for RPM.
To qualify for reimbursement, CMS expects providers to ensure they follow these remote patient monitoring requirements:
- Charge Medicare Part B patients a 20% percent copayment. While routinely waiving copays can trigger federal fines, CMS stated that healthcare providers can do so during the COVID-19 crisis to help clinicians care for their patients while mitigating the risk of the spread of the virus.
- Patients must consent — in writing or verbally — to receiving RPM services.
- The RPM service must be ordered by a physician or other “qualified healthcare professional,” such as a nurse practitioner, certified nurse specialist, or physician assistant.
- Patients must be monitored for at least 16 days to be applied to a billing period (a requirement to bill for CPT 99454).
- Data can be wirelessly synced for evaluation.
In addition, CMS stipulates that RPM devices must meet the U.S. Food and Drug Administration's definition of a medical device.
Remote Patient Monitoring CPT Codes: 4 Tips
Here are four tips to help ensure you use the four primary remote patient monitoring codes properly:
- A provider can only bill CPT 99454 once per patient every 30 days regardless of the number of devices used.
- Under CPT 99457, RPM can be performed by the billing physician, qualified healthcare professional, or clinical staff. It requires at least 20 minutes of logged management time each month.
- Once CPT 99457 has been billed, an organization can add up to two instances of CPT 99458 per month: once at 40 minutes and once at 60 minutes.
- A provider can bill via these RPM codes during the same service period as chronic care management (CCM) (via CPT codes 99487-99490), transitional care management (TCM) (via CPT codes 99495-99496), and behavioral health integration (BHI) (via CPT codes 99484, 99492-99494).
Changes to Remote Patient Monitoring CMS Rules Due to COVID-19
In the days and weeks that followed the declaration of COVID-19 as a pandemic and national health emergency, federal and state governments as well as private payers announced changes to rules intended to help improve access to care (i.e., reduce barriers to care). This change allowed patients who were under the restrictions of stay-at-home orders to reduce contact with others and maintain social distancing while still receiving essential care services.
On the healthcare delivery side, one of the more significant changes concerned CMS temporarily relaxing and expanding telehealth rules. Remote patient monitoring is a telehealth delivery system. In May 2020, CMS issued two Medicare physician fee schedule interim final rules that revised policies and requirements.
Four of the most noteworthy changes to remote patient monitoring policies in these interim final rules are as follows:
- Removal of the requirement that there must be an established patient-practitioner relationship to initiate the delivery of RPM services. New and established patients can receive RPM services.
- Clarification that RPM services can be used for physiologic monitoring of patients with acute and/or chronic conditions.
- Modification of the requirement that consent must be obtained prior to providing an initial remote physiologic monitoring service. Rather, practitioners can now obtain consent at the time services are provided and by individuals providing RPM services under contract to the ordering physician or qualified healthcare professional.
- Confirmation that RPM services can be furnished under general supervision.
CMS published a helpful resource answering frequently asked questions on Medicare fee-for-service billing that includes some questions about RPM. Access it here.
Rules for Remote Patient Monitoring in 2022
Here are four tips to help ensure you use the four primary remote patient monitoring codes properly:
- A provider can only bill CPT 99454 or 99455 once per patient every 30 days regardless of the number of devices used.
- Under CPT 99457, RPM can be performed by the billing physician, qualified healthcare professional, or clinical staff. It requires at least 20 minutes of logged management time each month.
- Once CPT 99457 has been billed, an organization can add up to two instances of CPT 99458 per month: once at 40 minutes and once at 60 minutes.
- A provider can bill via these RPM codes during the same service period as chronic care management (CCM) (via CPT codes 99487-99490), transitional care management (TCM) (via CPT codes 99495-99496), and behavioral health integration (BHI) (via CPT codes 99484, 99492-99494).
Changes to Remote Patient Monitoring CMS Rules Due to COVID-19
In the days and weeks that followed the declaration of COVID-19 as a pandemic and national health emergency, federal and state governments as well as private payers announced changes to rules intended to help improve access to care (i.e., reduce barriers to care). This change allowed patients who were under the restrictions of stay-at-home orders to reduce contact with others and maintain social distancing while still receiving essential care services.
On the healthcare delivery side, one of the more significant changes concerned CMS temporarily relaxing and expanding telehealth rules. Remote patient monitoring is a telehealth delivery system. In May 2020, CMS issued two Medicare physician fee schedule interim final rules that revised policies and requirements.
Four of the most noteworthy changes to remote patient monitoring policies in these interim final rules are as follows:
- Removal of the requirement that there must be an established patient-practitioner relationship to initiate the delivery of RPM services. New and established patients can receive RPM services.
- Clarification that RPM services can be used for physiologic monitoring of patients with acute and/or chronic conditions.
- Modification of the requirement that consent must be obtained prior to providing an initial remote physiologic monitoring service. Rather, practitioners can now obtain consent at the time services are provided and by individuals providing RPM services under contract to the ordering physician or qualified healthcare professional.
- Confirmation that RPM services can be furnished under general supervision.
CMS published a helpful resource answering frequently asked questions on Medicare fee-for-service billing that includes some questions about RPM. Access it here.
Rules for Remote Patient Monitoring in 2022
The 2021 Medicare physician fee schedule final rule included many significant changes to remote patient monitoring (i.e., remote physiological monitoring) and the provision of other remote services.
RPM-related topics affected by the final rule that apply in 2022 included the following:
- Definition of "interactive communication"
- Device requirements
- Established patient-physician relationship requirement following the public health emergency
- Timing of patient consent
- Furnishing of services by auxiliary personnel
- Eligibility of patients with acute conditions
- Requirement measurement-days to bill for RPM
- Designation of RPM devices as an expense
You can read what CMS states about these topics and more here.
What to Know About CPT 99091
This remote patient monitoring CPT code requires an additional caveat. Up until the 2021 final rules, organizations could still code with the provider-specific CPT 99091 but rarely did so since the newer RPM codes discussed above were almost always the better option. The 2021 rule declared that 99091 could be billed in addition to the newer care management codes, such as CPT 99457.
However, the new interpretation issued by CMS in the final rule essentially permits providers to bill for an extra "complex" RPM management service when the provider must spend significant time managing a patient and their RPM care plan. Since the 2021 rule change, CPT 99091 can be billed each 30 days whenever complex management occurs without affecting the ability to bill clinical staff time via CPT 99457 each calendar month.
Clarification for Remote Patient Monitoring 2021 Rules
The initial 2021 final rule had quite a few confusing and contradictory statements. In reaction to this, less than two months after the final 2021 rule was issued, CMS took the unusual step to issue a correction document. This document served to clarify a number of areas of confusion concerning RPM billing requirements. These areas are as follows:
- Activities covered under CPT 99457 and 99458
- Single practitioner delivery of RPM services
- The number of measurement-days required for billing CPT 99453 and 99454 (i.e., "16-day requirement" vs. "2-day requirement"
The correction document can be accessed here. A helpful summary of key takeaways is available here.
Remote Patient Monitoring Audits: Importance of Compliance
Understanding and following proper RPM coding and billing rules is essential to not only getting paid what you deserve but also to ensuring you maintain compliance with rules and regulations. RPM compliance has taken on even greater importance with the January 2021 announcement that CMS would be conducting audits of Medicare Part B telehealth services in two phases. RPM is one of the services included in the second phase.
How can providers of RPM services find themselves in auditing hot water? There are those organizations that choose to intentionally violate rules in an effort to make more money. These scenarios tend to be rare. Rather, most RPM compliance problems stem from either misunderstanding requirements, such as those described above, or engaging with RPM vendor partners that cut corners, either unintentionally or intentionally. You can learn more about the decision by CMS to begin auditing RPM and areas that will likely be focused on by auditors here.
Now that your coding and reimbursement questions have hopefully been answered, it’s necessary to examine the final consideration: How do you choose a software system that will fit your organization?
Comments
0 comments
Article is closed for comments.