Summary of Coding and Billing for CCM:
Initial CCM Coding Distinctions: Practitioners utilize CPT 99490 for at least 20 minutes of clinical staff time and CPT 99491 for at least 30 minutes of personal physician or qualified healthcare professional time. Both codes require the management of at least two chronic conditions expected to last 12 months or until death.
Strategic Use of Add-On Codes: capture additional care time beyond initial thresholds using CPT 99439 for staff-led services and CPT 99437 for provider-led services. These codes allow organizations to bill for increments of care that exceed the standard monthly allotments.
Complex CCM Requirements: Complex CCM (CPT 99487) addresses patients requiring moderate or high complexity medical decision making. This code requires 60 minutes of clinical staff time, with CPT 99489 available for each additional 30-minute increment of care provided.
Strict Billing Exclusivity: Only one practitioner receives reimbursement per patient for CCM services in any given calendar month. Furthermore, a practitioner must report either non-complex or complex CCM for a specific patient; both cannot be billed simultaneously for the same service period.
Heightened Audit Oversight: The OIG closely scrutinizes CCM reimbursement to investigate potential overpayment and incorrect billing. Consistent adherence to CMS rules and precise documentation are the primary defenses against federal auditing.
2026 Reimbursement Growth: The 2026 Physician Fee Schedule final rule delivered a significant increase in reimbursement for chronic disease management services. Success requires a commitment to reviewing annual rate tables, as geographic pricing and work RVUs fluctuate yearly.
Comprehensive Care Plan Necessity: All CCM billing depends on the establishment, implementation, revision, or monitoring of a comprehensive care plan. This document serves as the clinical foundation for all non-face-to-face coordination services.
The federal government has been increasingly supportive of care management programs. However, it is also more closely scrutinizing chronic care management reimbursement. It's important to ensure that you appropriately and consistently follow the rules of CCM codes and CCM billing. Expect more auditing to investigate causes of overpayment associated with incorrect billing of the service (more about this later in the chapter).
Rules for CPT 99490 and the Other Chronic Care Management Codes
Let's explore the most common and frequently used chronic care management CPT codes.
CPT 99490 and CPT 99491: Initial CCM Codes
We start our discussion about chronic care management coding and billing with the basic chronic care management CPT code, introduced in 2015, and its sister CPT code, which became effective in 2019. Together, these two CCM codes are sometimes referred to as the non-complex CCM codes.
CPT 99490 Chronic care management services, at least 20 minutes of clinical staff time directed by a physician or other qualified healthcare professional, per calendar month, with the following required elements:
- Multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient.
- Chronic conditions place the patient at significant risk of death, acute exacerbation/ decompensation, or functional decline.
- Comprehensive care plan established, implemented, revised, or monitored.
CPT 99490 assumes 15 minutes of work by the billing practitioner each month.
CPT 99491 Chronic care management services, provided personally by a physician or other qualified healthcare professional, at least 30 minutes of physician or other qualified health care professional time, per calendar month, with the following required elements:
- Multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient.
- Chronic conditions place the patient at significant risk of death, acute exacerbation/ decompensation, or functional decline.
- Comprehensive care plan established, implemented, revised, or monitored.
Difference Between CPT 99490 and CPT 99491
The between CPT 99490 and CPT 99491 is subtle but significant. Under CPT 99490, clinical staff supervised by a physician or other qualified healthcare professional can perform CCM for billing purposes. CPT 99491, on the other hand, compensates physicians or other qualified healthcare professionals for time spent on CCM-related care and requires them to provide such care personally. CPT 99491 also requires a minimum of 30 minutes a month of CCM versus the 20 minutes required as per CPT 99490.
CPT 99439 and CPT 99437: CCM Add-On Codes
These are two CCM add-on codes: CPT 99439, which replaced HCPCS code G2058 in 2021, and CPT 99437, which were added for 2022 in the 2022 Medicare Physician fee schedule final rule.
CPT 99439 Chronic care management services, each additional 20 minutes of clinical staff time directed by a physician or other qualified healthcare professional, per calendar month.
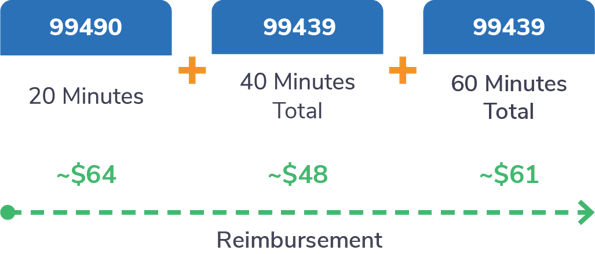
When to Report CPT 99439
As an add-on code for CPT 99491, it should only be billed for time spent beyond the initial 30 minutes spent providing services under 99491.
CPT 99487: Initial Complex CCM Code
Introduced in 2017 when the CCM benefit was expanded, this is a more complex CCM code. As we define in our glossary and noted earlier in this guide, complex CCM is intended for those patients with "two or more qualifying conditions who require more clinical staff and physician time" than non-complex CCM. In other words, these are patients who must also require moderate- to high-complexity medical decision-making. Let's look at the main CCM code.
CPT 99487 Complex chronic care management services, with the following required elements:
- Multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient
- Chronic conditions place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline
- Establishment or substantial revision of a comprehensive care plan
- Moderate or high complexity medical decision making
- 60 minutes of clinical staff time directed by a physician or other qualified healthcare professional, per calendar month
CPT 99489: Complex CCM Add-On Code
Now let's look at the add-on code to CPT 99487.
CPT 99489 Each additional 30 minutes of clinical staff time directed by a physician or other qualified health care professional, per calendar month (list separately in addition to code for primary procedure).
When to Report CPT 99489
As the end of the description for CPT 99489 suggests, this code should not be listed on its own. Rather, report in conjunction with CPT 99487 when a patient requires an additional 30 minutes of care in the month. This comes on top of the 60 minutes already covered under CPT 99487.
2023 Chronic Care Management CPT Codes
| CPT Code | Service | Staff Type | Care Management Time | Billing Units/Month (Max) | Reimbursement |
| 99490 | CCM | Clinical | First 20 minutes | 1 | ~$63 |
| 99439 | CCM | Clinical | Each additional 30 minutes | 2 | ~$48 |
| 99491 | CCM | Physician or qualified healthcare professional | At least 30 minutes | 1 | ~$85 |
| 99437 | CCM | Physician or qualified healthcare professional | Each additional 30 minutes | No limit | ~$60 |
| 99487 | Complex CCM | Clinical | First 30 minutes | 1 | ~$133 |
| 99849 | Complex CCM | Clinical | Each additional 30 minutes | No limit | ~$70 |
Other Relevant Care Management Codes
In addition to these chronic care management codes, there are complementary services that are often billed with CCM by organizations that have developed a comprehensive care management program. Three examples are remote physiological monitoring (sometimes referred to as remote patient monitoring or RPM), behavioral health integration (BHI) care management services, and, less frequently, principal care management (PCM). Read more about these codes here or reference this helpful CMS resource. You can also learn more by reading this Medical Economics column written by Prevounce's Daniel Tashnek.
OIG Audit Reveals Chronic Care Management Overpayments
In mid-2021, the federal Office of Inspector General (OIG) conducted an audit covering nearly 8 million claims submitted by physicians and more than 240,000 claims submitted by hospitals for non-complex and complex chronic care management services provided in 2017 and 2018.
The results of this audit have short- and long-term implications for providers of CCM services as well as software vendors. Here are the most important things to understand about the audit and its consequences:
- Why OIG performed the CCM audit — The agency specifically focused on whether payments made by the Centers for Medicare & Medicaid Service (CMS) for the two types of chronic care management services — non-complex and complex — during 2017 and 2018 complied with federal requirements. As OIG notes, "CCM services are a relatively new category of Medicare-covered services and are at higher risk for overpayments." This audit expands on the findings of a previous audit that found CMS lacked sufficient controls to effectively ensure Medicare payments for non-complex CCM services during 2015 and 2016 complied with federal requirements.
- What the latest chronic care management audit found — The audit determined that there were nearly $2 million in overpayments associated with about 50,000 claims for non-complex and complex chronic care management services rendered during 2017 and 2018. From these claims, beneficiaries' cost sharing totaled up to about $541,000. According to OIG, the overpayment errors were attributed to CMS lacking claim system edits to prevent and detect overpayments.
- What OIG recommended — Among several recommendations from the agency, these are some of the standouts:
- Direct Medicare contractors to recover the overpayments within the reopening period.
- Instruct providers to refund up to ~$541,000 which beneficiaries were required to pay.
- Notify appropriate providers to exercise reasonable diligence in identifying, reporting, and returning overpayments in accordance with the 60-day rule. The 60-day rule, created by the Affordable Care Act, requires providers to use reasonable diligence to identify overpayments via proactive compliance activities to monitor overpayments and investigate potential overpayments in a timely manner.
- Implement claim system edits to prevent and detect future overpayments for chronic care management services.
Considering Medicare's plans to support the growth of CCM, the audit's results suggest that CMS will be stepping up its oversight of the chronic care management program. What does this mean for practitioners? You'll need to step up your oversight as well and better ensure you are coding and billing properly — or face potential violation penalties. Keeping your CCM program compliant is not difficult, but it requires you to be mindful of the requirements when you set up your clinical and administrative workflows. Choosing a CCM software provider that makes compliance a top priority is extra insurance during periods of increased scrutiny and change.
Comments
0 comments
Article is closed for comments.